Normally, the aortic valve has three flaps (leaflets) that regulate blood flow by opening and closing, allowing blood to flow throughout your body.
Aortic valve disease occurs when the aortic valve doesn’t work properly; it either fails to close tightly (aortic regurgitation or insufficiency) or gets too tight (aortic stenosis).
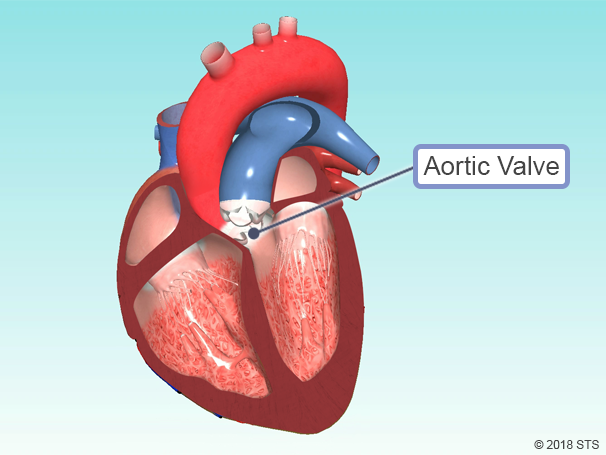

In a healthy aortic valve, valve leaflets open wide to let blood through and close tightly to keep it from going backward. The valve leaflets are thin and pliable.

There are two main types of aortic valve disease:
- Aortic Regurgitation (also known as aortic insufficiency) — the valve does not close completely, allowing blood to leak backward into the heart
- Aortic Stenosis — the valve is too tight and does not open enough to allow blood to leave the heart and spread to the body

The aortic valve may be abnormal from birth (congenital), or it could become diseased with age (acquired).
The most common congenital aortic valve abnormality, called a bicuspid aortic valve, occurs when the valve has only two leaflets (bicuspid) instead of three (tricuspid). This prevents the valve from opening or closing completely. Although the abnormality has been there since birth, symptoms may not be felt until adulthood. Your physician may be able to hear distinctive murmurs (abnormal sounds that can be heard with a stethoscope) when listening to your heart.

Copyright: alila/123RF Stock Photo
Acquired aortic valve disease occurs because your valve simply wears out over time, and usually happens as you age. Calcium collects on the valve and can cause the leaflets to stiffen and narrow, which limits their motion.
If the aorta—the main blood vessel coming out of the heart—is diseased, this also can lead to problems with the aortic valve.
A faulty or failing aortic valve may cause symptoms such as shortness of breath, chest pain, and dizziness or loss of consciousness (passing out). These symptoms are due to the heart having to work harder because of the narrowed or leaky valve.
Early on, these symptoms may be noticeable only when exercising, but as the disease progresses, you could experience shortness of breath with minimal or no activity.
Some patients will be unable to sleep flat in bed or may awaken short of breath. Another potential symptom is swollen feet, particularly in the late afternoon or early evening.
There is no one test that can diagnose aortic valve disease, so your doctor may recommend one or more of the following: electrocardiogram (EKG), echocardiogram (echo), chest x-ray, blood tests, and coronary angiography. For more information on these tests, visit our common diagnostic tests page.
Currently, NO MEDICATION can cure aortic valve disease, so it is most commonly treated with surgery.
Aortic stenosis can only be treated with aortic valve replacement. Sometimes, aortic valves that are leaking (regurgitant) can be repaired. Your Heart Team—you, your medical team, and your cardiothoracic surgeon—will determine the best treatment option for you based on your symptoms and test results. You can print these sample questions to use as a basis for discussion with your doctor.
You also can access the STS Risk Calculator, which can help calculate your risk of death or other complications from open heart surgery. The results can help you and your doctor to determine the best course of treatment.
SURGICAL TREATMENT OPTIONS FOR AORTIC VALVE DISEASE









The STS mission is to advance cardiothoracic surgeons’ delivery of the highest quality patient care through collaboration, education, research, and advocacy.