Determining the optimal surgical approach for early-stage non-small cell lung cancer (NSCLC) has grown more complex with increasing use of sublobar resection. Recent randomized trials show comparable outcomes to lobectomy in carefully selected patients, but questions remain about real-world application.
A new expert consensus document from the Society of Thoracic Surgeons (STS), published in The Annals of Thoracic Surgery and developed by the Workforce on Evidence-Based Surgery and a panel of thoracic surgeons, provides guidance on the use of sublobar resection.
The recommendations focus on patient selection, margin requirements, and lymph node evaluation, offering a practical framework for clinical decision-making.
“These expert consensus statements are designed to provide real-world, practical recommendations,” said Onkar Khullar, MD, a thoracic surgeon at Emory University, who chaired the panel. “At the same time, we hope they place some guard rails around which patients are truly appropriate for sublobar resection, so that this technique is used appropriately, effectively, and safely.”
Bridging Evidence and Practice
The recommendations were developed through a comprehensive literature review and a modified Delphi process, requiring greater than 75% agreement for each statement. The panel reached consensus on 21 statements across seven key areas of controversy, including:
- Sublobar resection versus lobectomy
- Wedge versus segmentectomy
- Central tumor location
- High-risk histologic features
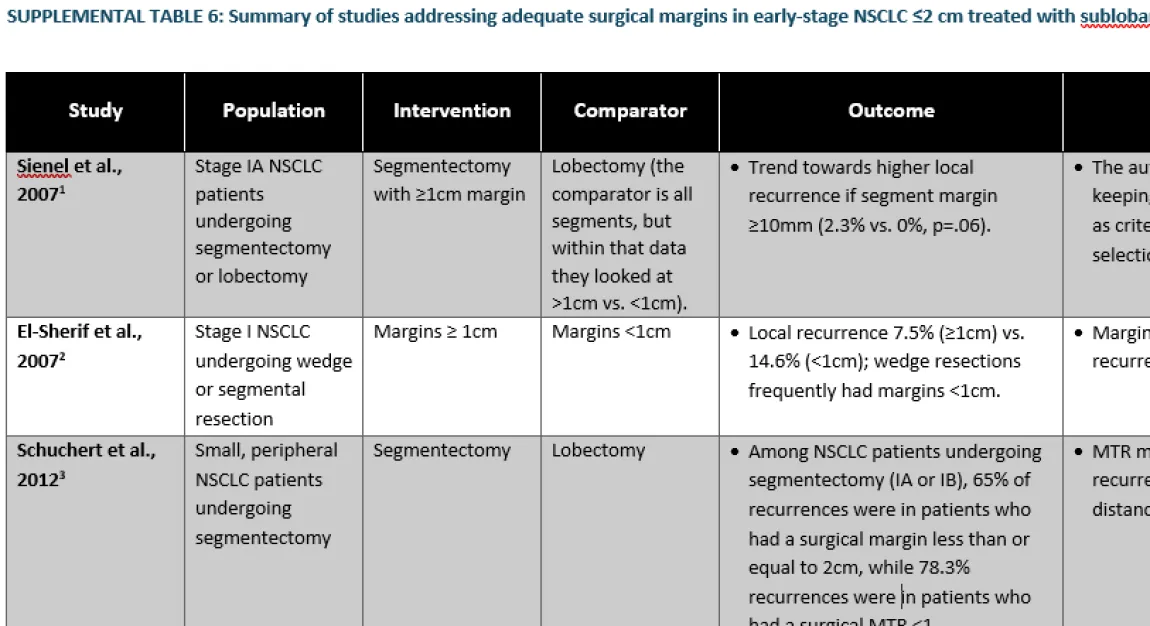
- Adequate margins
- Complex segmentectomy
- Intraoperative lymph node assessment
A major gap identified was the difference between randomized trial criteria and real-world practice, particularly in lymph node staging. In randomized trials, only patients with pathologically confirmed negative nodes were included, which is not always practical in real-world settings, where it may not be feasible to perform intraoperative frozen sections on all nodes.
To address this, the panel recommends proceeding with sublobar resection when preoperative staging is negative and nodes are not clinically suspicious, while maintaining intraoperative vigilance.
“If a surgeon becomes suspicious of a lymph node during the operation, they should perform a frozen analysis,” Dr. Khullar stated. “If that is positive, consideration should be given to converting to an anatomic resection.”
Key Recommendations
The consensus reinforces that sublobar resection—either segmentectomy or wedge resection—is an appropriate option for patients with peripheral, node-negative tumors measuring 2 cm or less, provided that adequate surgical margins and lymph node assessment can be achieved.
“Sublobar resection should be considered in patients with peripheral, node-negative tumors less than 2 cm if, and only if, appropriate margins and lymph node evaluation can be obtained,” Dr. Khullar noted. “If those criteria cannot be met, and the patient is a candidate for lobectomy, then lobectomy remains the best option.”
The document emphasizes the importance of margin quality, recommending a minimum 10 mm margin for solid tumors and supporting intraoperative frozen section analysis to guide decision-making. It also notes that while segmentectomy is often considered a more anatomic approach, it may involve longer operative times and greater complexity, which should be weighed in older patients or those with limited pulmonary reserve.
Unresolved Questions
Despite growing evidence supporting sublobar resection, important uncertainties remain—particularly regarding high-risk tumor features such as spread through air spaces (STAS), lymphovascular invasion (LVI), and visceral pleural invasion (VPI).
“The biggest gap in current knowledge is whether sublobar resections should be performed in patients with high-risk pathology features,” Dr. Khullar explained. “First, we often cannot identify these features before surgery. Second, even if we do, it’s unclear whether sublobar resection is appropriate.”
Current consensus suggests there is insufficient evidence to recommend routine conversion to lobectomy based on these findings alone. To address this gap, new data fields have been incorporated into the STS General Thoracic Surgery Database, with the goal of generating more robust evidence in the future.
Informing Surgical Decision-Making
As sublobar resection use expands, the panel expects these recommendations to standardize care while maintaining clinical flexibility. The hope is that these statements will influence how surgeons approach case selection, margin assessment, and lymph node evaluation in everyday practice.
Although further research is needed—particularly to refine patient selection and clarify high-risk features—the consensus provides an important foundation for early-stage NSCLC care..
“As more data become available, we expect these recommendations to evolve,” Dr. Khullar added. “But for now, they offer a practical framework to ensure patients receive the most appropriate surgical treatment.”