Discover the featured content in this month’s The Annals of Thoracic Surgery issue, personally selected by Editor-in-Chief Dr. Joanna Chikwe & Senior Editor Dr. Robbin Cohen, who highlight the authors' important findings, with select illustrations from Dr. Sarah Chen, Associate Editor/CMI. As an additional benefit to your STS Membership and Annals subscription, this monthly newsletter aims to bring expert perspectives on recently published research, straight to your digital doorstep.
Featured in the August 2026 issue...
STS Document | The Society of Thoracic Surgeons 2026 Clinical Practice Guidelines for the Prevention and Treatment of New-Onset Postoperative Atrial Fibrillation After Cardiac Surgery
Chatterjee, Schena, and coauthors
The STS Workforce on Evidence-Based Surgery convened a multidisciplinary writing group to synthesize contemporary evidence and develop guidelines for preventing and treating new-onset postoperative atrial fibrillation (POAF) after cardiac surgery. Fifteen recommendations were developed around three primary domains:
- Perioperative strategies to reduce POAF, including preventive medications (beta-blockers, amiodarone, calcium channel blockers, anti-inflammatory agents) and electrolyte management.
- Intraoperative strategies, including posterior pericardiotomy, bi-atrial pacing, and prophylactic injection of botulinum toxin into epicardial fat pads.
- Postoperative treatment regarding rate versus rhythm control and cardioversion.
-Robbin Cohen, MD, MMM
Senior Editor
Lung | A Society of Thoracic Surgeons General Thoracic Surgery Database Analysis of the Association Between Lymph Node Dissection and Chylothorax
Kamtam, Shrager, and coauthors
This retrospective analysis of the STS General Thoracic Surgery Database studied 152,823 patients who underwent lung resection for stage 1-3 non-small cell lung cancer between 2015 and 2024. Chylothorax occurred in 1,110 patients (0.73%) and was associated with a higher rate of major morbidity (35.7% vs 6.6%, P < .001) but not increased mortality (1.4% vs 1%, P = .17) when compared with patients who did not develop chylothorax. Predictors of chylothorax included the number of sampled lymph nodes, number of lymph node stations, right-sided tumor, dialysis, open surgical approach, and 2R sampling.
-Robbin Cohen, MD, MMM
Senior Editor
Lung | Is Sublobar Resection Optimal for Peripheral Nodules ≤2cm with Micropapillary or Solid Histologic Components?
Xu, Luo, and coauthors
This retrospective single-center study compared outcomes of lobectomy vs sublobar resection in 501 patients with <2 cm peripheral adenocarcinomas containing micropapillary or solid histologic components between 2018 and 2020. Lobectomy was associated with higher 5-year recurrence-free survival and lung cancer-specific survival compared with sublobar resection (log-rank P < .001). In matched analysis, consolidation to tumor ratio >0.5, visceral pleural invasion, wedge resection, and segmentectomy were independently associated with worse lung cancer-specific survival and recurrence-free survival compared with lobectomy.
-Robbin Cohen, MD, MMM
Senior Editor
Coronary | Hybrid Revascularization With Robotic Totally Endoscopic Coronary Bypass and Stents: What Are the Outcomes When The Stent Does Not Happen?
Nisivaco, Balkhy, and coauthors
This 12-year retrospective single center study compared 332 patients (80%) who completed a hybrid coronary revascularization strategy—totally endoscopic coronary bypass (TECAB) plus percutaneous coronary intervention (PCI)—with 85 patients (20%) who had TECAB but failed to have subsequent PCI. Multivessel TECAB was performed in most patients in both groups with bilateral internal thoracic artery use in approximately 90%. Incomplete PCI most commonly involved right coronary artery or nondominant circumflex lesions. At 5 years, cardiac survival was similar between the two groups (95.7% complete PCI group vs 95.4% incomplete PCI, log-rank P = .608). Freedom from cardiac mortality, myocardial infarction, repeated revascularization, and major adverse cardiac and cerebrovascular events was also not significantly different.
-Robbin Cohen, MD, MMM
Senior Editor
Valve | Optimal Management for Moderate Aortic Stenosis at the Time of Coronary Artery Bypass Grafting
Yu, Hartman, and coauthors
The STS Adult Cardiac Surgery Database was utilized to compare isolated CABG (8,922 pts, 48.9%) with CABG plus SAVR (9,325 pts, 51.1%) in patients with moderate aortic stenosis (aortic valve (AV) mean gradient 20-40 mm HG, AV area 1-1.5 cm2). Isolated CABG patients tended to be older and have more co-morbidities and were more likely to present with myocardial infarction. Though risk adjusted mid-term outcomes showed similar all-cause mortality, patients who underwent isolated CABG were at increased risk for mid-term readmission for heart failure and AV intervention. Rate of AV intervention at 8 years for CABG vs CABG + SAVR was 25.9% vs 2.4% respectively.
-Robbin Cohen, MD, MMM
Senior Editor
Valve | Trends in Utilization and Outcomes of Ross, Transcatheter and Surgical Aortic Valve Replacement in Adults Younger Than 65 Years Old
Alabbadi, Egorova, and coauthors
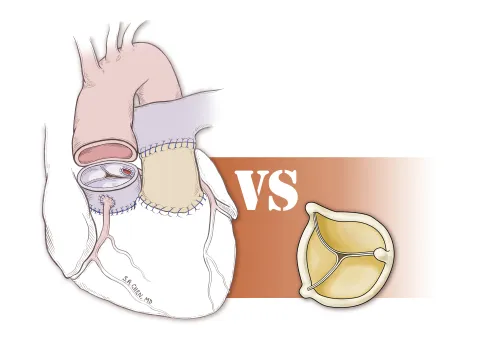
California and New York discharge data from 2000-2025 was reviewed to identify patients under 65 years who underwent Ross, TAVR, SAVR-mech, or SAVR-bio. Ross use declined from 2000-2005 but rebounded to 2.8% by 2022. The median age of Ross patients was significantly lower than the other three procedures. Median follow-up was 7.7 years after Ross, 3.2 years after TAVR, 8.8 years after SAVR-Bio, and 12 years after SAVR-mech. In hospital mortality was low across all cohorts. At 6 years, unadjusted survival after TAVR was slightly lower than bio SAVR, (96.2% v. 97.2%, P = .1), higher after SAVR-mech (97.6%, P < .001), and highest after Ross (99.5%, P < .001). Six year aortic valve reintervention rate was highest after Ross, followed by SAVR-mech, SAVR-bio, and TAVR. TAVR was associated with higher mortality, infective endocarditis, and heart failure hospitalization compared with SAVR-bio. SAVR-mech showed higher risks of infective endocarditis, myocardial infarction, heart failure, and pacemaker implantation compared with SAVR-bio.
-Robbin Cohen, MD, MMM
Senior Editor
Transplant & Mechanical Support | Extracorporeal Life Support for Post-Cardiotomy Acute Right Ventricular Failure: A Retrospective Observational Multicenter Study
Bianchi, Lorusso, and coauthors
This retrospective analysis from the Multi-institutional Post-Cardiotomy Extracorporeal Life Support (PELS-1) study compared 240 acute right ventricular failure (aRVF) patients (12%) with 1770 patients (88%) who received post-cardiotomy extracorporeal life support (ECLS) for other indications. Patients with aRVF had more preoperative right sided dysfunction, and more frequently underwent tricuspid valve procedures and aortic root operations. They required longer ECLS support and longer ICU stays than ECLS for other indications. Despite more complications and persistent right sided heart failure, both in-hospital survival (aRVF 59%, other indications 61%, P = .526) and long-term survival were comparable.
-Robbin Cohen, MD, MMM
Senior Editor
Aorta | Definitive Repair After Staged Hybrid Procedure of the Ascending Aorta and Aortic Valve Redo Surgery for Kinked Aortic Graft
Chaugle, Byrne, and coauthors
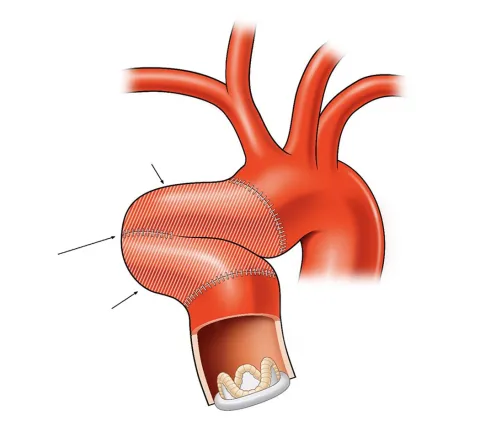
The authors describe a patient who underwent aortic valve replacement (AVR) and replacement of the ascending aorta, who 6 years later developed symptomatic kinking of the redundant ascending aortic graft. This was treated with endovascular repair of the kinked graft. Four years later, the patient developed symptomatic prosthetic aortic stenosis which was not amenable to TAVR. As a result, open excision of the endograft, repeat AVR, and revision of the ascending aortic graft was successfully performed.
-Robbin Cohen, MD, MMM
Senior Editor
Coronary | Open vs Intact Pleura During Internal Thoracic Artery Harvesting: A Meta-Analysis of Randomized Trials
Ingason, Gaudino, and coauthors
This meta-analysis looked at 9 randomized trials that compared open vs closed pleural techniques during internal thoracic artery harvesting for CABG in a total of 1869 patients (1015 open, 854 closed). The closed technique was associated with less pleural effusion, less pulmonary atelectasis, less impairment of FEV1, and shorter postoperative ventilation time. The closed technique was also associated with lower chest tube drainage at 24 hours postop, lower operative mortality, but more postoperative tamponade. Click the link to read the full manuscript, as well as my invited commentary.
-Robbin Cohen, MD, MMM
Senior Editor