Determining the optimal management strategy for pleural mesothelioma (PM) remains one of the most challenging areas in thoracic oncology. As a rare and aggressive malignancy, PM requires careful coordination of diagnostic, surgical, and systemic therapies. While surgery has historically played a central role, its benefit continues to be debated.
The Society of Thoracic Surgeons (STS) 2026 Expert Consensus on the Multimodal Treatment of Pleural Mesothelioma, developed by a multidisciplinary panel and published in The Annals of Thoracic Surgery, provides updated recommendations on the multimodal management of PM, with particular emphasis on the role of surgical intervention.
Bridging Evidence and Real-World Practice

A key challenge addressed in the document is the gap between clinical evidence and real-world outcomes. According to lead author Jeffrey Velotta, MD, of Kaiser Permanente Oakland Medical Center, that gap is often driven by differences in surgical experience. “The biggest divide is between general thoracic surgeons and those with high-volume mesothelioma experience,” Velotta said, noting that outcomes are closely tied to disease-specific expertise and case volume. He emphasized that many studies and guidelines do not fully account for this variability. “Mesothelioma-specific experience—not just general surgical skill—can significantly impact outcomes,” he added.
Refining Diagnosis and Staging
A central theme of the recommendations is the importance of accurate diagnosis and staging. The panel strongly emphasizes that adequate pleural biopsy is essential for confirming histologic subtype, which directly influences prognosis and treatment decisions.
In addition, the consensus highlights the critical role of advanced imaging:
- CT and PET imaging: Required at a minimum to assess disease extent.
- Multidisciplinary Tumor Board (MTB): Essential for treatment planning, involving surgeons, oncologists, radiologists, and pathologists with specific PM expertise.
Multimodal Therapy as the Standard Approach
The consensus emphasizes that PM treatment should integrate surgery with systemic therapies such as chemotherapy, immunotherapy, or radiation. When evaluating surgical candidates, the panel suggests focusing on several key clinical indicators:
- Histologic subtype: Greatest benefit is seen in epithelioid, localized disease; outcomes remain poorer for sarcomatoid and biphasic subtypes.
- Performance status: A patient's overall functional ability is an independent prognostic indicator.
- Physiologic reserve: Careful assessment of cardiopulmonary function and nutritional levels.
- Case volume: Surgery should be concentrated in high-volume centers with documented experience in PM management.
“Patients benefit most from a multimodal approach that combines surgery with systemic therapy,” Velotta said.
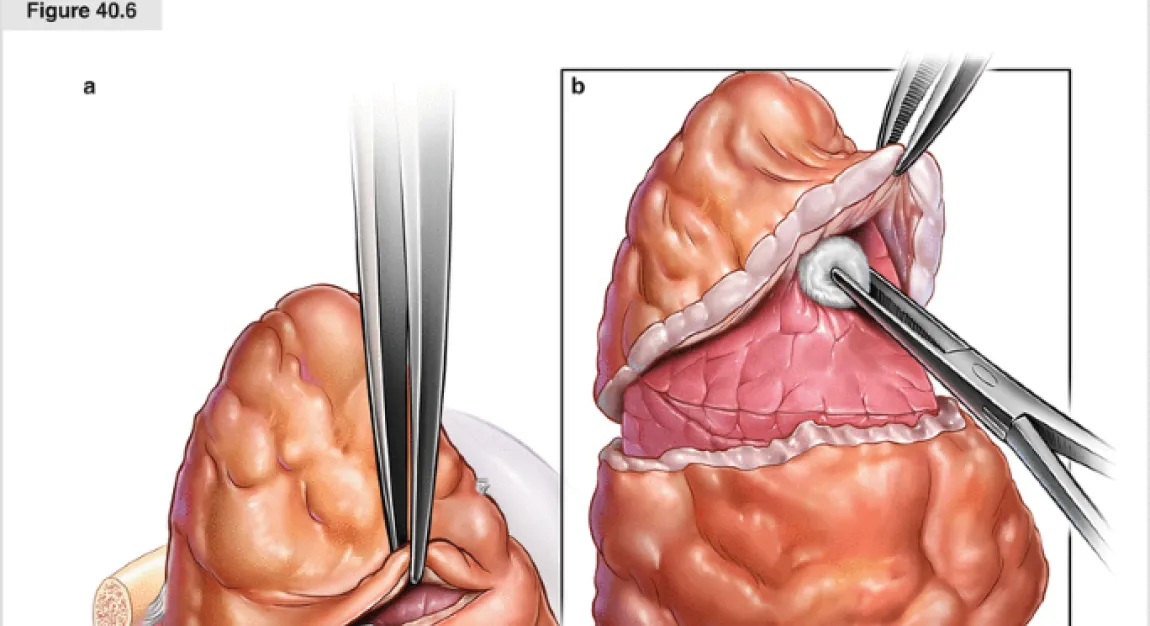
Surgical Approach: Moving Toward Lung-Sparing Techniques
One of the most definitive recommendations is the strong preference for lung-sparing surgical techniques. Pleurectomy/decortication (P/D) and extended P/D (EPD) are favored over extrapleural pneumonectomy (EPP), which carries higher morbidity without a clear survival advantage in contemporary studies. “Lung-sparing surgery, when performed in experienced centers, can offer meaningful long-term benefits with acceptable risk,” Velotta noted.
Treatment Sequencing and Ongoing Uncertainty
Therapy sequencing remains an area of active debate, with both neoadjuvant and adjuvant approaches considered reasonable. Velotta highlighted two key unanswered questions: “We still don’t know whether chemotherapy is best given before or after surgery, and whether intraoperative adjuncts should be used routinely.”
Recent data, including the MARS-2 trial, have also questioned the overall benefit of surgery, though the panel emphasizes ongoing controversy related to trial design and differences in surgical expertise.
A Framework for Complex Decision-Making
As treatment strategies for pleural mesothelioma continue to evolve, the STS consensus provides a structured yet flexible framework for clinicians. While acknowledging gaps in high-quality evidence, the panel emphasizes the importance of expertise, multidisciplinary care, and individualized treatment planning which includes surgery in a multimodal regimen to optimize patient outcomes.