The ongoing opioid crisis has led to a marked increase in tricuspid valve endocarditis (TVE), particularly among people who inject drugs (PWID). This trend presents cardiac surgeons with complex clinical and psychosocial challenges, as patients often face overlapping issues—including infection, addiction, and social instability. These factors complicate surgical decision-making and underscore the need for comprehensive, multidisciplinary approaches to care.
To address the lack of clear surgical guidance and the unique challenges associated with TVE in PWID, the Society of Thoracic Surgeons (STS) convened a multidisciplinary panel to develop expert consensus statements focused on clinical decision-making in this high-risk population.
“Unlike left-sided endocarditis, TVE lacks definitive data to guide surgical timing and intervention strategies,” said Joshua Goldberg, MD, of Weill Cornell Medicine, who chaired the task force that produced the document. “This consensus document represents an important step forward, organizing expert recommendations into key categories that reflect the multifaceted clinical challenges encountered in managing PWID with TVE. Each group of statements addresses specific, real-world dilemmas faced by the multidisciplinary care team.”
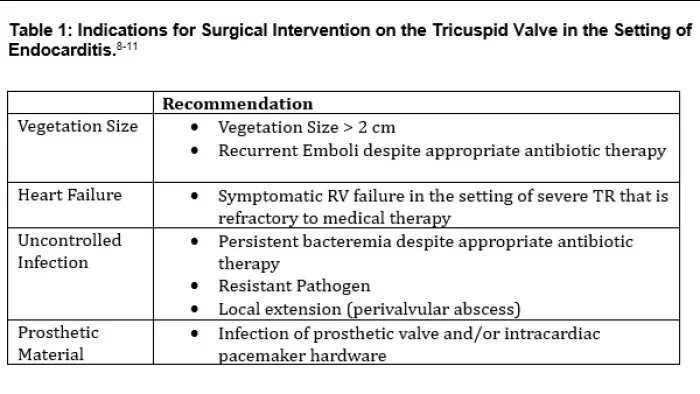
The eight core categories outlined in the document include:
Vegetation size
Influence of microbial organism on surgical decisions
Management of persistent bacteremia and timing of antibiotics
Prosthetic valve infection
Decisions around valve removal, repair, or replacement
Prosthetic type selection
Use of emerging technologies such as transcatheter debulking
Ethical challenges of recurrent disease in the context of substance use
A Thorough, Multidisciplinary Approach to Consensus Building
The STS writing group employed a rigorous, evidence-based methodology to develop the consensus statements, incorporating a comprehensive literature review and a modified Delphi process. The evidence review was guided by PICO Framework (Patients/Population, Intervention, Comparison/Control, Outcome)-formatted questions, ensuring a structured and focused appraisal of the data. Consensus statements were established in the first round of voting, with a minimum threshold of 75% agreement required from a multidisciplinary panel that included cardiac surgeons and infectious disease specialists
Navigating Complex Decisions in Endocarditis
“First, surgeons and treatment teams must always remember that tricuspid endocarditis in the setting of injection drug use is a symptom and sign of the disease of addiction. Effective care requires addressing both the infection and the underlying pathology of addiction,” said Dr. Goldberg. “Second, published surgical indications for tricuspid valve surgery are largely extrapolated from data derived from studies on left-sided valve disease. When combined with complex psychosocial factors, the decision to operate can be enigmatic and is best approached through thoughtful, multidisciplinary evaluation.”
A Practical Framework for Attentive, Evidence-Informed Care
Ultimately, this expert consensus provides cardiac surgeons with a practical, evidence-informed framework for managing TVE in PWID. It supports individualized decision-making while promoting standardization in key areas such as vegetation assessment and the use of emerging technologies. Most importantly, it emphasizes the need for compassionate, team-based care that integrates medical, surgical, and psychosocial perspectives. The document serves not only as a clinical tool, but also as a call to action—to treat not just the infection, but the patient as a whole.
In addition to offering clinical guidance, the consensus highlights critical knowledge gaps that demand further investigation. “Because published surgical indications are largely extrapolated from studies on left-sided valve disease, the true indications and optimal timing for intervention remain unclear—particularly in the absence of uncontrolled sepsis or right heart failure,” Dr. Goldberg noted. “We also lack a clear understanding of the efficacy and utility of transcatheter therapies, which have seen a dramatic rise in use in recent years.”
Determining the optimal management strategy for pleural mesothelioma (PM) remains one of the most challenging areas in thoracic oncology. As a rare and aggressive malignancy, PM requires careful coordination of diagnostic, surgical, and systemic therapies. While surgery has historically played a central role, its benefit continues to be debated.
The Society of Thoracic Surgeons (STS) 2026 Expert Consensus on the Multimodal Treatment of Pleural Mesothelioma, developed by a multidisciplinary panel and published in The Annals of Thoracic Surgery, provides updated recommendations on the multimodal management of PM, with particular emphasis on the role of surgical intervention.
Bridging Evidence and Real-World Practice
Image
Dr. Jeffrey Velotta
A key challenge addressed in the document is the gap between clinical evidence and real-world outcomes. According to lead author Jeffrey Velotta, MD, of Kaiser Permanente Oakland Medical Center, that gap is often driven by differences in surgical experience. “The biggest divide is between general thoracic surgeons and those with high-volume mesothelioma experience,” Velotta said, noting that outcomes are closely tied to disease-specific expertise and case volume. He emphasized that many studies and guidelines do not fully account for this variability. “Mesothelioma-specific experience—not just general surgical skill—can significantly impact outcomes,” he added.
Refining Diagnosis and Staging
A central theme of the recommendations is the importance of accurate diagnosis and staging. The panel strongly emphasizes that adequate pleural biopsy is essential for confirming histologic subtype, which directly influences prognosis and treatment decisions.
In addition, the consensus highlights the critical role of advanced imaging:
CT and PET imaging: Required at a minimum to assess disease extent.
Multidisciplinary Tumor Board (MTB): Essential for treatment planning, involving surgeons, oncologists, radiologists, and pathologists with specific PM expertise.
Multimodal Therapy as the Standard Approach
The consensus emphasizes that PM treatment should integrate surgery with systemic therapies such as chemotherapy, immunotherapy, or radiation. When evaluating surgical candidates, the panel suggests focusing on several key clinical indicators:
Histologic subtype: Greatest benefit is seen in epithelioid, localized disease; outcomes remain poorer for sarcomatoid and biphasic subtypes.
Performance status: A patient's overall functional ability is an independent prognostic indicator.
Physiologic reserve: Careful assessment of cardiopulmonary function and nutritional levels.
Case volume: Surgery should be concentrated in high-volume centers with documented experience in PM management.
“Patients benefit most from a multimodal approach that combines surgery with systemic therapy,” Velotta said.
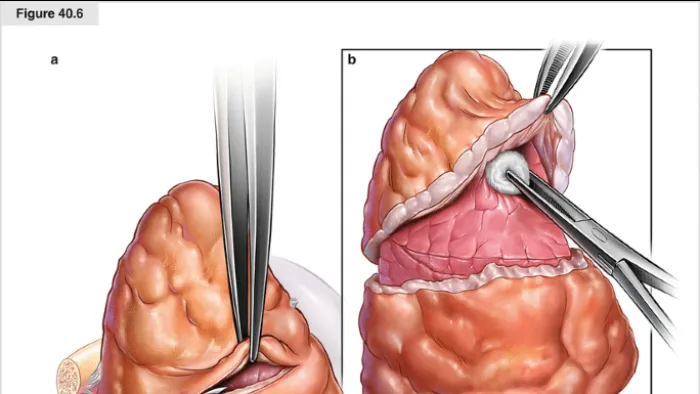
One of the most definitive recommendations is the strong preference for lung-sparing surgical techniques. Pleurectomy/decortication (P/D) and extended P/D (EPD) are favored over extrapleural pneumonectomy (EPP), which carries higher morbidity without a clear survival advantage in contemporary studies. “Lung-sparing surgery, when performed in experienced centers, can offer meaningful long-term benefits with acceptable risk,” Velotta noted.
Treatment Sequencing and Ongoing Uncertainty
Therapy sequencing remains an area of active debate, with both neoadjuvant and adjuvant approaches considered reasonable. Velotta highlighted two key unanswered questions: “We still don’t know whether chemotherapy is best given before or after surgery, and whether intraoperative adjuncts should be used routinely.”
Recent data, including the MARS-2 trial, have also questioned the overall benefit of surgery, though the panel emphasizes ongoing controversy related to trial design and differences in surgical expertise.
A Framework for Complex Decision-Making
As treatment strategies for pleural mesothelioma continue to evolve, the STS consensus provides a structured yet flexible framework for clinicians. While acknowledging gaps in high-quality evidence, the panel emphasizes the importance of expertise, multidisciplinary care, and individualized treatment planning which includes surgery in a multimodal regimen to optimize patient outcomes.
Postoperative atrial fibrillation (POAF) remains the most common complication following cardiac surgery—and a persistent challenge for clinicians seeking consistent, evidence-based management. In response, the Society of Thoracic Surgeons (STS) has released new clinical practice guidelines, now published in The Annals of Thoracic Surgery, outlining a comprehensive, surgery-specific framework for the prevention and treatment of POAF.
A Multidisciplinary, Evidence-Driven Effort
Co-led by Subhasis Chatterjee, MD, of Baylor College of Medicine, and Stefano Schena, MD, PhD, of Medical College of Wisconsin, the STS 2026 Clinical Practice Guidelines for the Prevention and Treatment of New-Onset Postoperative Atrial Fibrillation after Cardiac Surgery were developed through a multidisciplinary effort by the STS Workforce on Evidence-Based Surgery. The group evaluated contemporary evidence to generate practical, consensus-based recommendations focused specifically on the prevention and treatment of POAF after cardiac surgery.
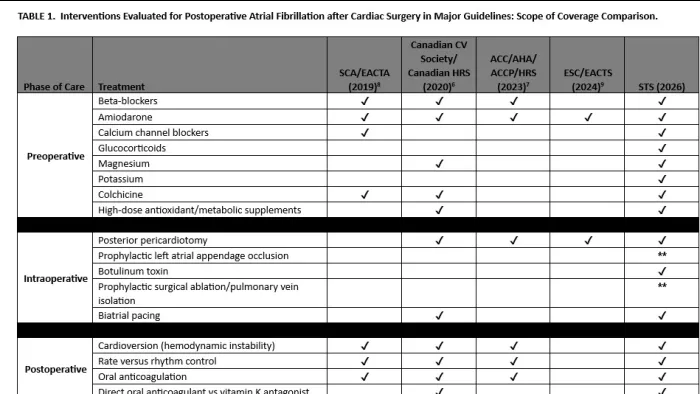
A Phase-Based Framework Across the Surgical Continuum
The document establishes a phase-based framework spanning the preoperative, intraoperative, and postoperative periods. Drawing from randomized and observational studies, the panel graded recommendations using standardized methods aligned with American Association for Thoracic Surgery (AATS), European Association for Cardio-Thoracic Surgery (EACTS), European Society of Thoracic Surgeons (ESTS), and STS harmonization guidelines.
A central theme of the guidelines is transparency around uncertainty and a focus on meaningful patient outcomes. “One of the goals of these guidelines was not to promote a single dominant therapy, but to provide a structured, phase-based approach that can reduce unwarranted practice variation while still allowing clinical judgment,” said Dr. Chatterjee. He emphasized that POAF should be viewed as a marker of perioperative vulnerability rather than an isolated rhythm disturbance, helping to identify patients at higher risk for complications and future atrial arrhythmias. This perspective supports targeted surveillance and follow-up rather than reflexive escalation of therapy.
The guidelines also underscore that POAF is distinct from preexisting atrial fibrillation, with different mechanisms, natural history, and management implications. Core strategies include careful rhythm monitoring, early rate or rhythm control, and individualized anticoagulation decisions. At the same time, the document acknowledges ongoing uncertainty regarding optimal anticoagulation timing and duration, arrhythmia burden, and the role of adjunctive surgical interventions.
Addressing Uncertainty and Variability in Practice
Dr. Schena noted that the guideline development process highlighted the variability in clinical practice and the limitations of available evidence. “The time spent discussing and reviewing helped us recalibrate our stance and recognize how limited the evidence truly is for many commonly used interventions,” he said. While no single strategy eliminates POAF, he emphasized that its clinical impact can be reduced through a combination of measures applied across all phases of care. He also noted that the long-term implications of POAF in patients without prior atrial fibrillation remain uncertain and must be weighed against individual patient risk factors.
Together, these guidelines provide a pragmatic framework that clinicians can apply across the surgical continuum. By emphasizing evidence-based practices, acknowledging uncertainty, and discouraging ineffective interventions, the document aims to support informed clinical decision-making and improve outcomes for patients undergoing cardiac surgery.
In the season two premiere episode of Thinking Thoracic, cohosts Drs. Erin Gillaspie, Hari Keshava, Jeff Yang, and Jane Yanagawa review the latest thoracic surgery research presented at the 2026 STS Annual Meeting in New Orleans.
NEW ORLEANS—February 1, 2026— Ascending aortic hemiarch reconstruction offers the same long-term benefits to patients over age 65 with acute type A aortic dissection (ATAAD) as more complex extended arch reconstruction procedures, according to a study presented today at the 2026 Society of Thoracic Surgeons Annual Meeting.
NEW ORLEANS—January 31, 2026— A late-breaking study leveraging more than 1.5 million patient records from The Society of Thoracic Surgeons Adult Cardiac Surgery Database found that coronary artery bypass grafting (CABG) performed off-pump by experienced surgeons is associated with significantly lower perioperative morbidity and mortality compared with on-pump CABG, while long-term survival outcomes were largely equivalent across techniques.
NEW ORLEANS—January 31, 2026—A nationwide, real-world analysis using the STS General Thoracic Surgery Database (GTSD) from 2012 to 2023, analyzed 16,056 adults who underwent esophagectomy for primary esophageal cancer to develop and validate a long-term all-cause mortality risk model.
NEW ORLEANS—January 31, 2026—A late-breaking study drawing on more than 15 years of national outcomes data from the STS Adult Cardiac Surgery Database (ACSD) suggests that the two most commonly used multi-arterial coronary artery bypass grafting (CABG) strategies—bilateral internal thoracic artery (BITA) and single internal thoracic artery plus radial artery (SITA+RA)—offer comparable long-term survival overall, with important differences emerging by patient age.
NEW ORLEANS—January 31, 2026—Breakthrough research presented at the 2026 Society of Thoracic Surgeons Annual Meeting shows that additional lymph node evaluation is needed during surgery for non-small cell lung cancer (NSCLC) to accurately identify cancer spread.
On Friday, Jan. 30, at 9:30 a.m., Stephanie Worrell, MD, of the University of Arizona, presented STS Perforation Guidelines during the "Esophageal Perforation Management" session. Her talk introduced a new Society of Thoracic Surgeons (STS) Expert Consensus Document designed to improve the diagnosis and management of esophageal perforation, a rare but potentially fatal condition.
Image
Dr. Stephanie Worrell
Esophageal perforation, often a complication of endoscopic procedures, requires early diagnosis, as mortality and morbidity increase if treatment is delayed beyond 24 hours. Despite advances in treatment, management remains inconsistent due to the condition’s rarity and limited clinical data.
To address this gap, the STS convened a multidisciplinary panel of thoracic surgeons and gastroenterologists, who reviewed studies from the past 14 years to develop consensus statements on diagnosis, treatment, and long-term care. For stable patients with confirmed perforation, the consensus supports endoscopic therapies when matched appropriately to anatomy and operator expertise. Surgical intervention remains essential for unstable patients or complex cases.
In her talk, Dr. Worrell discussed how the guidelines provide clarity in clinical scenarios that often prompt uncertainty. “These recommendations clarify when further investigation is appropriate and when it’s safe to observe or discharge,” she said. She notes that the guidelines are particularly valuable for conditions like spontaneous pneumomediastinum where further workup may be unnecessary. Additionally, there is now strong data for CT esophagrams and growing evidence for endoscopic approaches that are not yet used consistently.
During the Airway Issues session on Friday, Jan. 30 at 1:30 p.m., Joseph Nellis, MD, of Duke University Medical Center, will present the Richard E. Clark Memorial Paper, Impact of Preoperative Tracheostomy on Outcomes Following Congenital Cardiac Surgery: A Study of the STS Congenital Heart Surgery Database, at STS 2026. In this presentation, Dr. Nellis will examine how preoperative tracheostomy affects outcomes following congenital cardiac surgery, an area with limited prior data despite longstanding concerns about risk in this population.
Image
Dr. Joseph Nellis
Congenital cardiac surgery patients with preoperative tracheostomy represent a small but increasingly recognized group with complex medical needs. To better understand how tracheostomy status influences surgical outcomes, Dr. Nellis and colleagues analyzed national registry data spanning a decade of congenital cardiac operations, comparing patients with preoperative tracheostomy to those without this airway history.
Overall, patients with preoperative tracheostomy experienced higher rates of postoperative complications, readmissions, and mortality compared with those without tracheostomy. Even after accounting for differences in baseline risk, preoperative tracheostomy remained associated with an increased likelihood of infection-related complications and early mortality, though it was not linked to longer hospital stays or higher overall morbidity.
In his presentation, Dr. Nellis will outline the implications these findings inform risk stratification and surgical planning for children with complex airway and cardiac disease. He emphasizes that while preoperative tracheostomy identifies a higher-risk patient population, it should not, by itself, exclude patients from consideration for definitive congenital cardiac surgery.
NEW ORLEANS—January 29, 2026—At the 2026 Society of Thoracic Surgeons (STS) Annual Meeting, investigators will present a late-breaking study focused on surgical aortic valve replacement (SAVR) following prior transcatheter aortic valve replacement (TAVR), a clinical scenario increasingly encountered as TAVR use expands. The analysis draws on data from the STS Adult Cardiac Surgery Database to characterize risk over time and to validate a dedicated STS risk model designed to support decision-making for patients requiring surgery after TAVR.