The ongoing opioid crisis has led to a marked increase in tricuspid valve endocarditis (TVE), particularly among people who inject drugs (PWID). This trend presents cardiac surgeons with complex clinical and psychosocial challenges, as patients often face overlapping issues—including infection, addiction, and social instability. These factors complicate surgical decision-making and underscore the need for comprehensive, multidisciplinary approaches to care.
To address the lack of clear surgical guidance and the unique challenges associated with TVE in PWID, the Society of Thoracic Surgeons (STS) convened a multidisciplinary panel to develop expert consensus statements focused on clinical decision-making in this high-risk population.
“Unlike left-sided endocarditis, TVE lacks definitive data to guide surgical timing and intervention strategies,” said Joshua Goldberg, MD, of Weill Cornell Medicine, who chaired the task force that produced the document. “This consensus document represents an important step forward, organizing expert recommendations into key categories that reflect the multifaceted clinical challenges encountered in managing PWID with TVE. Each group of statements addresses specific, real-world dilemmas faced by the multidisciplinary care team.”
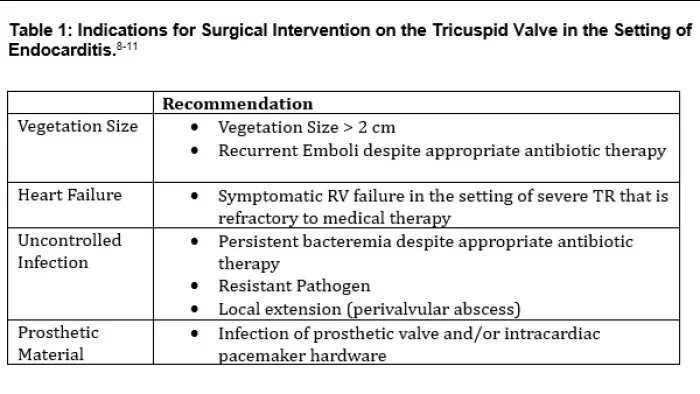
The eight core categories outlined in the document include:
- Vegetation size
- Influence of microbial organism on surgical decisions
- Management of persistent bacteremia and timing of antibiotics
- Prosthetic valve infection
- Decisions around valve removal, repair, or replacement
- Prosthetic type selection
- Use of emerging technologies such as transcatheter debulking
- Ethical challenges of recurrent disease in the context of substance use
A Thorough, Multidisciplinary Approach to Consensus Building
The STS writing group employed a rigorous, evidence-based methodology to develop the consensus statements, incorporating a comprehensive literature review and a modified Delphi process. The evidence review was guided by PICO Framework (Patients/Population, Intervention, Comparison/Control, Outcome)-formatted questions, ensuring a structured and focused appraisal of the data. Consensus statements were established in the first round of voting, with a minimum threshold of 75% agreement required from a multidisciplinary panel that included cardiac surgeons and infectious disease specialists
Navigating Complex Decisions in Endocarditis
“First, surgeons and treatment teams must always remember that tricuspid endocarditis in the setting of injection drug use is a symptom and sign of the disease of addiction. Effective care requires addressing both the infection and the underlying pathology of addiction,” said Dr. Goldberg. “Second, published surgical indications for tricuspid valve surgery are largely extrapolated from data derived from studies on left-sided valve disease. When combined with complex psychosocial factors, the decision to operate can be enigmatic and is best approached through thoughtful, multidisciplinary evaluation.”
A Practical Framework for Attentive, Evidence-Informed Care
Ultimately, this expert consensus provides cardiac surgeons with a practical, evidence-informed framework for managing TVE in PWID. It supports individualized decision-making while promoting standardization in key areas such as vegetation assessment and the use of emerging technologies. Most importantly, it emphasizes the need for compassionate, team-based care that integrates medical, surgical, and psychosocial perspectives. The document serves not only as a clinical tool, but also as a call to action—to treat not just the infection, but the patient as a whole.
In addition to offering clinical guidance, the consensus highlights critical knowledge gaps that demand further investigation. “Because published surgical indications are largely extrapolated from studies on left-sided valve disease, the true indications and optimal timing for intervention remain unclear—particularly in the absence of uncontrolled sepsis or right heart failure,” Dr. Goldberg noted. “We also lack a clear understanding of the efficacy and utility of transcatheter therapies, which have seen a dramatic rise in use in recent years.”
Read the Annals article.