Postoperative atrial fibrillation (POAF) remains the most common complication following cardiac surgery—and a persistent challenge for clinicians seeking consistent, evidence-based management. In response, the Society of Thoracic Surgeons (STS) has released new clinical practice guidelines, now published in The Annals of Thoracic Surgery, outlining a comprehensive, surgery-specific framework for the prevention and treatment of POAF.
A Multidisciplinary, Evidence-Driven Effort
Co-led by Subhasis Chatterjee, MD, of Baylor College of Medicine, and Stefano Schena, MD, PhD, of Medical College of Wisconsin, the STS 2026 Clinical Practice Guidelines for the Prevention and Treatment of New-Onset Postoperative Atrial Fibrillation after Cardiac Surgery were developed through a multidisciplinary effort by the STS Workforce on Evidence-Based Surgery. The group evaluated contemporary evidence to generate practical, consensus-based recommendations focused specifically on the prevention and treatment of POAF after cardiac surgery.
A Phase-Based Framework Across the Surgical Continuum
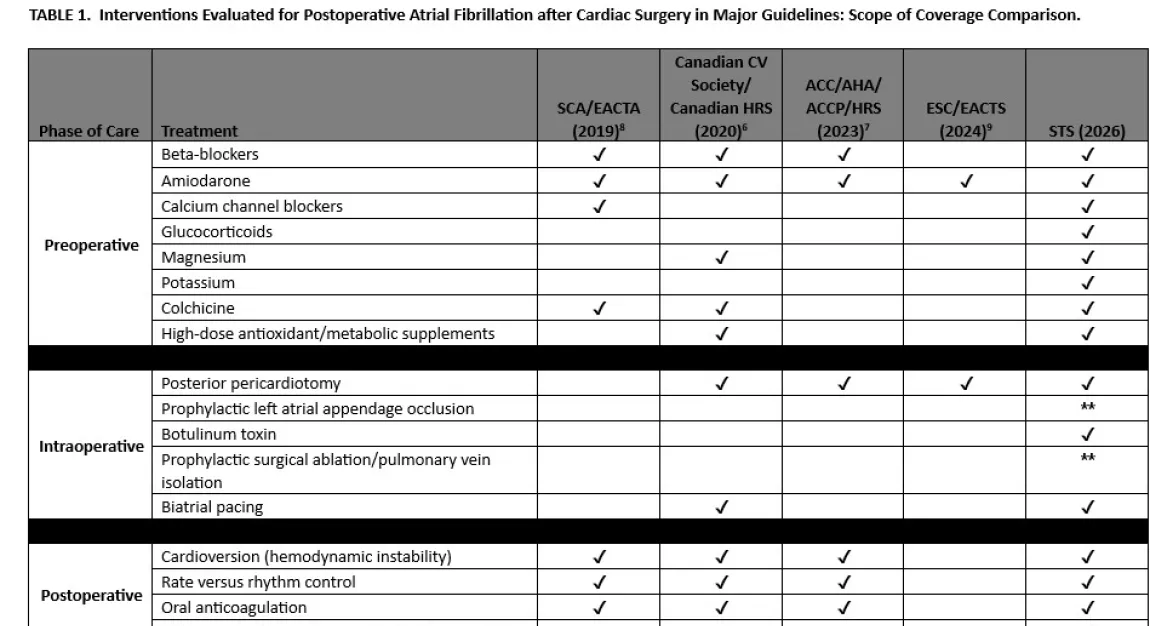
The document establishes a phase-based framework spanning the preoperative, intraoperative, and postoperative periods. Drawing from randomized and observational studies, the panel graded recommendations using standardized methods aligned with American Association for Thoracic Surgery (AATS), European Association for Cardio-Thoracic Surgery (EACTS), European Society of Thoracic Surgeons (ESTS), and STS harmonization guidelines.
A central theme of the guidelines is transparency around uncertainty and a focus on meaningful patient outcomes. “One of the goals of these guidelines was not to promote a single dominant therapy, but to provide a structured, phase-based approach that can reduce unwarranted practice variation while still allowing clinical judgment,” said Dr. Chatterjee. He emphasized that POAF should be viewed as a marker of perioperative vulnerability rather than an isolated rhythm disturbance, helping to identify patients at higher risk for complications and future atrial arrhythmias. This perspective supports targeted surveillance and follow-up rather than reflexive escalation of therapy.
The guidelines also underscore that POAF is distinct from preexisting atrial fibrillation, with different mechanisms, natural history, and management implications. Core strategies include careful rhythm monitoring, early rate or rhythm control, and individualized anticoagulation decisions. At the same time, the document acknowledges ongoing uncertainty regarding optimal anticoagulation timing and duration, arrhythmia burden, and the role of adjunctive surgical interventions.
Addressing Uncertainty and Variability in Practice
Dr. Schena noted that the guideline development process highlighted the variability in clinical practice and the limitations of available evidence. “The time spent discussing and reviewing helped us recalibrate our stance and recognize how limited the evidence truly is for many commonly used interventions,” he said. While no single strategy eliminates POAF, he emphasized that its clinical impact can be reduced through a combination of measures applied across all phases of care. He also noted that the long-term implications of POAF in patients without prior atrial fibrillation remain uncertain and must be weighed against individual patient risk factors.
Together, these guidelines provide a pragmatic framework that clinicians can apply across the surgical continuum. By emphasizing evidence-based practices, acknowledging uncertainty, and discouraging ineffective interventions, the document aims to support informed clinical decision-making and improve outcomes for patients undergoing cardiac surgery.