By Catherine T. Byrd, MD, H. Henry Guo, MD, PhD, and Natalie S. Lui, MD, MAS, from the Stanford University School of Medicine, California
STS News, Fall 2021 — The use of three-dimensional (3D) printing is expanding in cardiothoracic surgery. It can facilitate surgical planning and intraoperative guidance, be used to develop customized, implantable prostheses, and aid in patient and trainee education.
Although 3D printing for medical purposes is a fairly recent phenomenon, the process—additive manufacturing—has been in existence since the 1980s.
Additive Manufacturing
In additive manufacturing, very thin layers of material are deposited to form a 3D reconstruction of preoperative imaging. Thin slices (0.5 mm–1 mm) of a patient’s computed tomography or magnetic resonance imaging are optimal to gather details for the structure of interest.
The resulting images then undergo contouring and segmentation by a radiologist or technologist, who delineates structures of interest either manually or by using automated software. The data are then saved as a standard tessellation language (STL) file, essentially a series of triangles that convey the 3D nature of the anatomy. A surgeon may be involved to guide processing and highlight appropriate anatomy.
Next, the appropriate technique and materials are selected to print the model. Considerations include whether the material needs to be biocompatible and sterilizable because it will be implanted, or if the material needs similar mechanical properties as the native anatomy so that it can be used for education or simulation.
Models are then printed and undergo postprocessing, which involves removing any support structures requisite to the printing process, polishing, and additional steps such as dimensional verification and sterilization.
Operative Guidance
3D models can serve as beneficial tools for preoperative planning.
In 2019, a multidisciplinary team of cardiothoracic surgeons, radiologists, and engineers in Spain described its experience with 3D printing. Over the course of a year, the team printed 26 models of general thoracic pathology, including tracheal stenosis, chest wall tumors, carcinoid tumors, mediastinal tumors, and a Pancoast tumor. A majority of the surgeons surveyed (78%) stated that 3D models helped with preoperative planning, and 77% said that the models accurately represented the intraoperative experience. Specifically, during Pancoast tumor resections, 3D models may be used for preoperative planning and intraoperative reference, allowing surgeons to carefully select the operative approach and surgical instruments.
Other surgeons have reported that 3D models are an improvement over conventional radiographic imaging and may decrease operative times.
Customizable Prostheses
Customizable 3D printed prostheses also offer promise.
One example is using a customized carbon fiber prosthesis to shift mediastinal contents in postpneumonectomy syndrome. Theoretically, this could improve on conventional techniques using breast implants as these materials are easily distorted and can migrate or more rigid implants which may be difficult to insert intraoperatively.
Patient and Trainee Education
3D printed models also are great tools for patient education.
One randomized study examined using customized 3D printed models of stage I lung cancer and the surrounding transparent lung parenchyma during informed consent discussions. The model improved patient knowledge of the surgery but did not impact the ability to make an informed decision.
Resident procedural training can benefit from 3D printed models as well. One example of this involves a group of experienced and non-experienced cardiothoracic surgery residents, who were trained on 3D printed bronchoscopy models.
The time to intubate an ostium was very different between the two groups on pretesting. After training, both the experienced and inexperienced groups improved, and there was no difference in the final times to intubate an ostium between the experienced and non-experienced groups on post-testing, demonstrating the use of the bronchoscopy model to quickly close the experience gap.
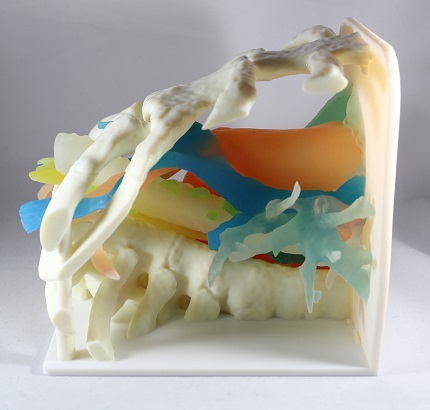
At our institution, cardiothoracic surgery residents use a 3D printed mediastinum model to learn mediastinoscopy. Those who train with this model are better able to identify normal anatomy and perform the procedure according to self-assessments and assessments by the supervising attending.
Promising Future
3D printing holds great promise in several aspects of our specialty. The many advantages include customizable patient-unique models, potential shortened procedure time, better patient understanding of diseased anatomy, and increased procedure confidence among surgical trainees.
More innovations will be seen as cardiothoracic surgeons explore 3D printing in their clinical, research, and education endeavors.