
STS News, Fall 2022 — With nearly as many women as men presenting with signs of ischemia in today’s health care settings, clinicians should keep in mind that coronary artery disease (CAD) goes beyond vessel obstruction, especially in female patients—and should take advantage of tools like advanced imaging to see past anatomic walls.
“More and more, I think we're recognizing that, when they’re designed for the identification of primarily obstructive CAD, conventional approaches can lead to repeated testing, especially in women,” said Viviany R. Taqueti, MD, MPH, from Brigham and Women’s Hospital in Boston, Massachusetts. “And yet, often without differentiating who’s truly at risk.”
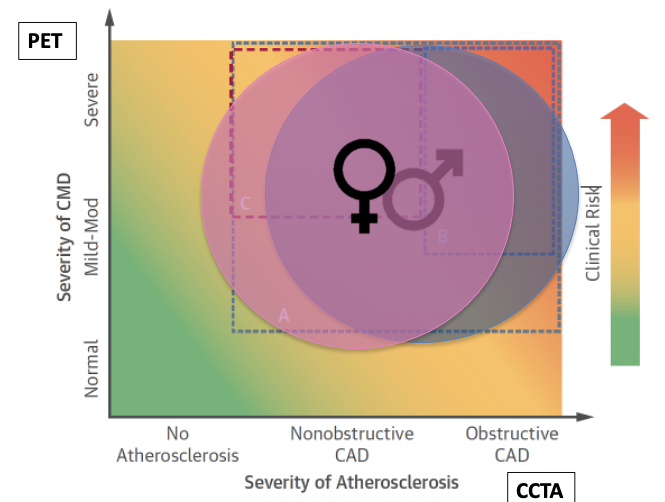
Obstructive CAD is just one phenotype of ischemic heart disease, and perhaps just the tip of the iceberg when physicians take into consideration the entirety of coronary circulation, Dr. Taqueti said. A physician needs to spot other pathologies such as diffuse non-obstructive CAD and coronary microvascular dysfunction, which can certainly impact patients’ cardiovascular outcomes, she explained.
As an example, Dr. Taqueti referred to a study in Denmark that presented observational data from a large registry of more than 11,000 patients who were referred for coronary angiography. The investigators found that up to a 32% of the male patients—and a startling 65% of female patients—had no significant obstructive disease to explain their symptoms.
“We need a more sophisticated toolbox that looks beyond regional wall motion abnormality or even regional perfusion abnormalities to consider and quantify absolute blood flow in the heart and quantify coronary flow reserve, or CFR,” said Dr. Taqueti.
Coronary microcirculation is of course too small to be directly imaged in vivo, and it needs to be evaluated indirectly by perturbing function. A variety of technologies make this possible.
"Conventional approaches can lead to repeated testing, especially in women. And yet, often without differentiating who’s truly at risk.”
In the invasive realm, historically, catheter-guided wire-based testing has provided measurements of CFR and microcirculatory resistance. But noninvasive methods, including cardiac magnetic resonance, Doppler ultrasound, and—the current gold standard—positron emission tomography, are revealing just how prevalent coronary microvascular dysfunction is in patients with angina or signs of ischemia.
Data from more angiography studies demonstrated that just under half of the patients had no obstructive disease. “And these were evaluated quite objectively, using fractional flow reserve normal values above 0.8,” Dr. Taqueti explained.
But from that group, a large majority—76% to 89%—had some evidence of objective coronary vasomotor dysfunction on testing.
“The vast majority of these had coronary microvascular dysfunction, with a minority having pure vasospasm,” said Dr. Taqueti. “This is important because we know that impaired flow reserves—that can certainly be manifestations of coronary microvascular disease—are associated with worse outcomes in terms of cardiac mortality in our patients.”
More revelations come with observational data that span multiple research centers: Even in patients with no obvious obstructive lesions or inducible ischemia on stress testing, impaired CFR is independently associated with major adverse events.
In those with significant obstructive CAD, CFR also modifies the outcome of coronary revascularization procedures, especially coronary artery bypass grafting (CABG), Dr. Taqueti pointed out. With long-term cardiovascular outcomes, patients with a severely reduced CFR who underwent CABG did as well as those with a preserved CFR to begin with (adjusted p for interaction = 0.03), suggesting that impaired CFR may serve as a marker for CABG benefit akin to diabetes or SYNTAX score, said Dr. Taqueti.
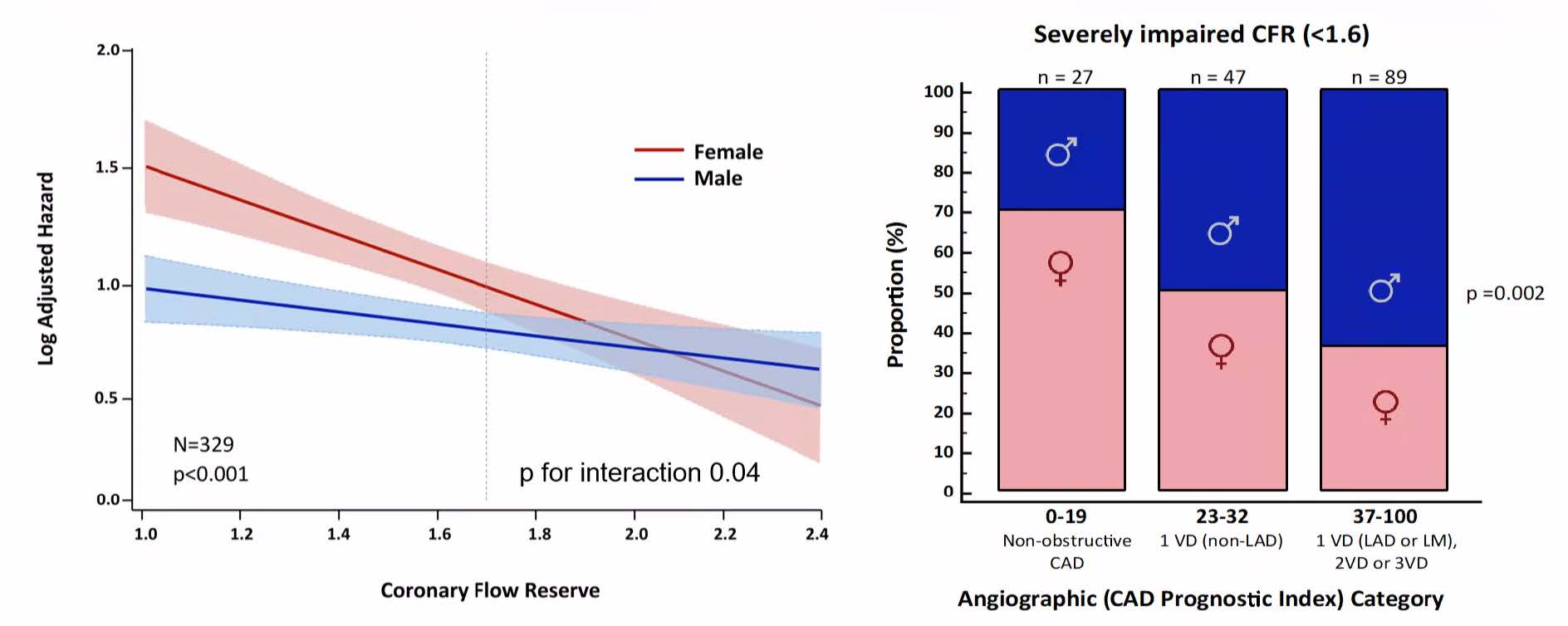
In women, severely impaired CFR appears to be even more prognostically significant. “You can see the divergence of the hazard for men and women with a significant interaction for sex as CFR values fall substantially below 2,” Dr. Taqueti explained. “Women appear to fare even worse at the very low range of CFR despite the fact that, when you look at anatomic findings, they are much less likely to have multivessel obstructive disease. In contrast, men were much more likely to have impaired CFR in the presence of multivessel disease—perhaps explaining their impaired flow reserves.”
Dr. Taqueti encouraged physicians to consider how these factors reframe their approach to understanding CAD, and to emphasize appropriate diagnostic testing to identify risk, which can help to curb repeated conventional testing in patients at low risk.
These recommendations were presented as part of the STS Coronary Conference this summer, in a session devoted to noninvasive diagnostic techniques for evaluation of high-risk ischemic heart disease. The conference united faculty and attendees from 18 countries with a multidisciplinary approach.
Course director Marc Ruel, MD, MPH, who serves as STS Canadian Director, touted the camaraderie displayed by participants of all backgrounds. “Surgeons have to be the top experts at understanding the very reason why they operate—or not—on a patient,” Dr. Ruel said. “It comes down to much more than ‘I can do this,’; rather, it should be ‘It is a good idea to be doing this for the patient, and I have the skills to do it.’ The Coronary Conference aimed to achieve this: Expert knowledge and skills in the huge, knowledge-intensive area of coronary surgery.”
Strong surgeons need strong cardiologists, anesthesiologists, radiologists, and other experts, Dr. Ruel said. “This is why we made the Coronary Conference so multidisciplinary and team-based, with a focus both on advanced practical knowledge and on advanced technical skills.”
“We need to understand microvascular disease in order to better treat ischemia in both women and men,” Dr. Taqueti added. “Coronary microvasculature represents an exciting new frontier in cardiovascular disease reduction, and the future is pointing toward a role for coronary microcirculation in macrovessel disease prognosis. That’s something we need to think about in all our practices.”